Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinic Development
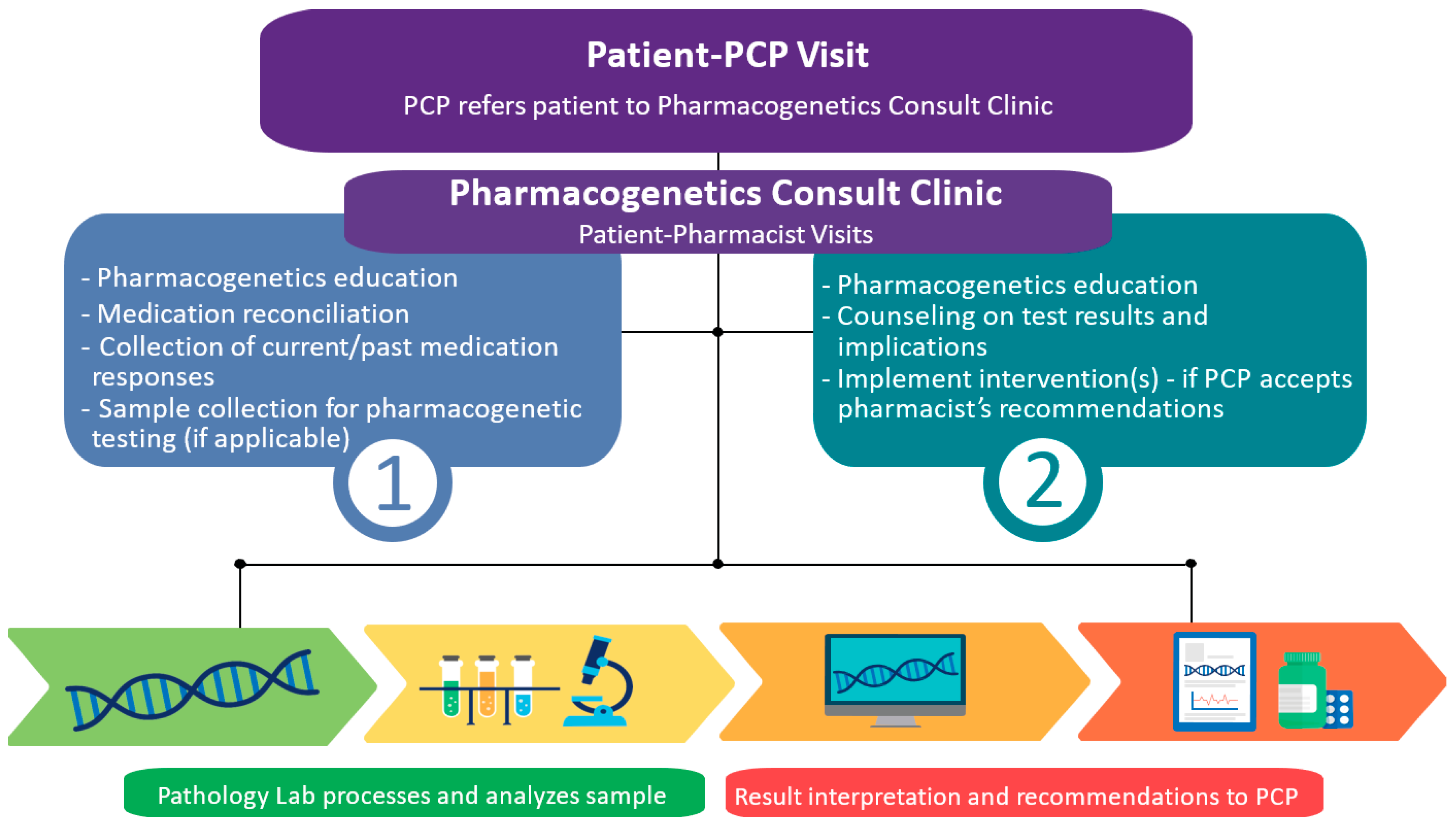
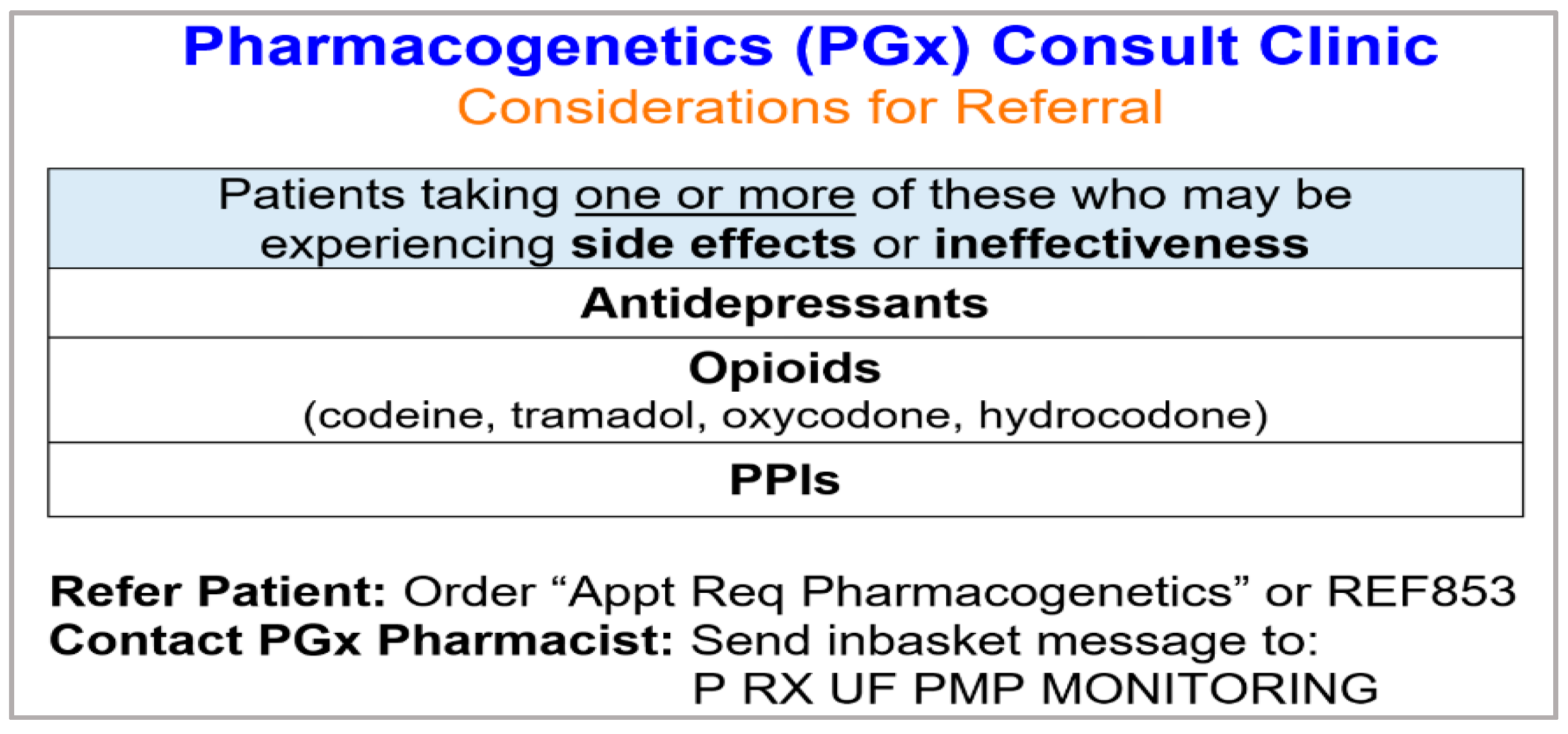
2.2. Clinic Workflow
3. Results
3.1. Medication Utilization
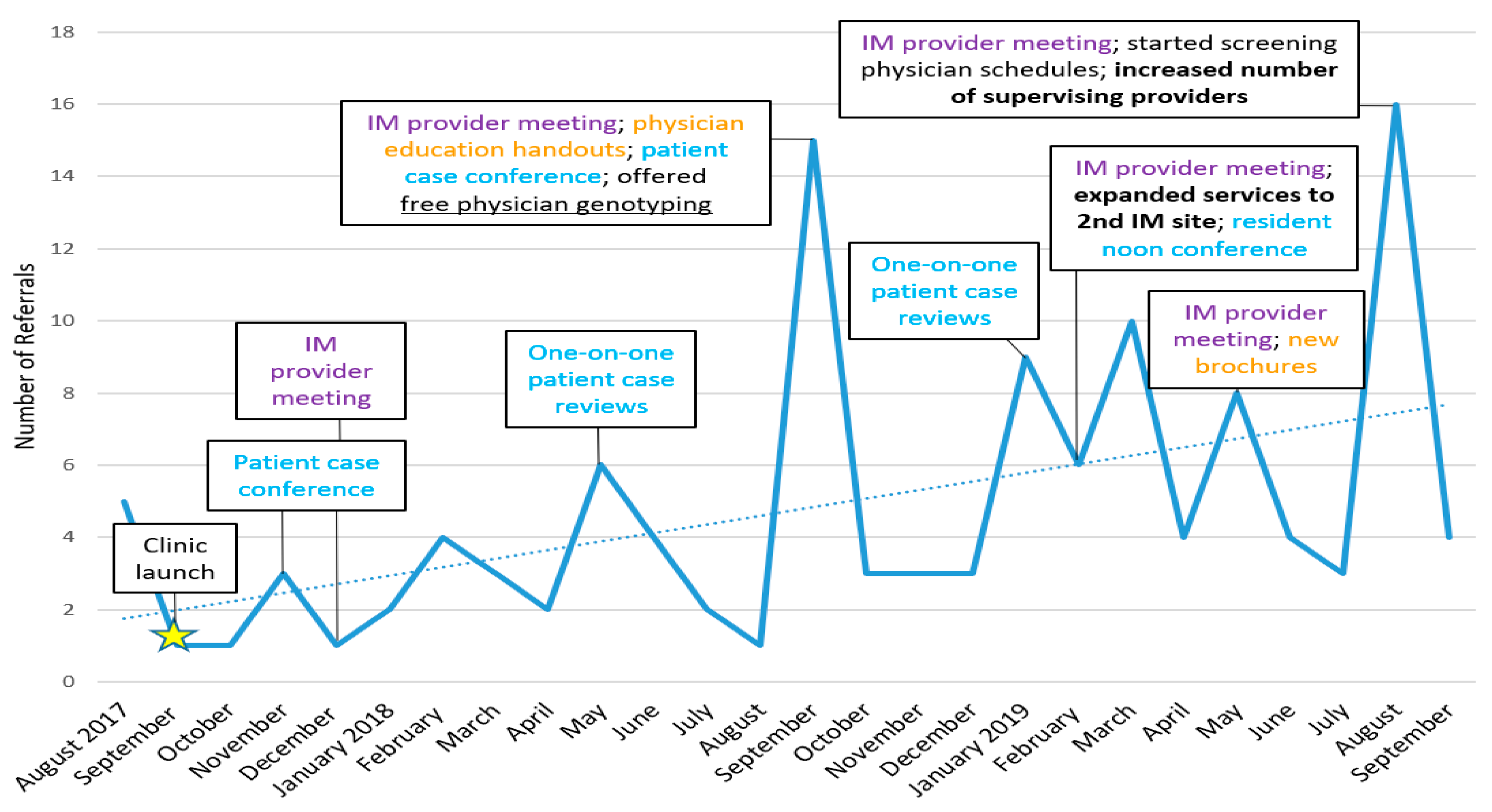
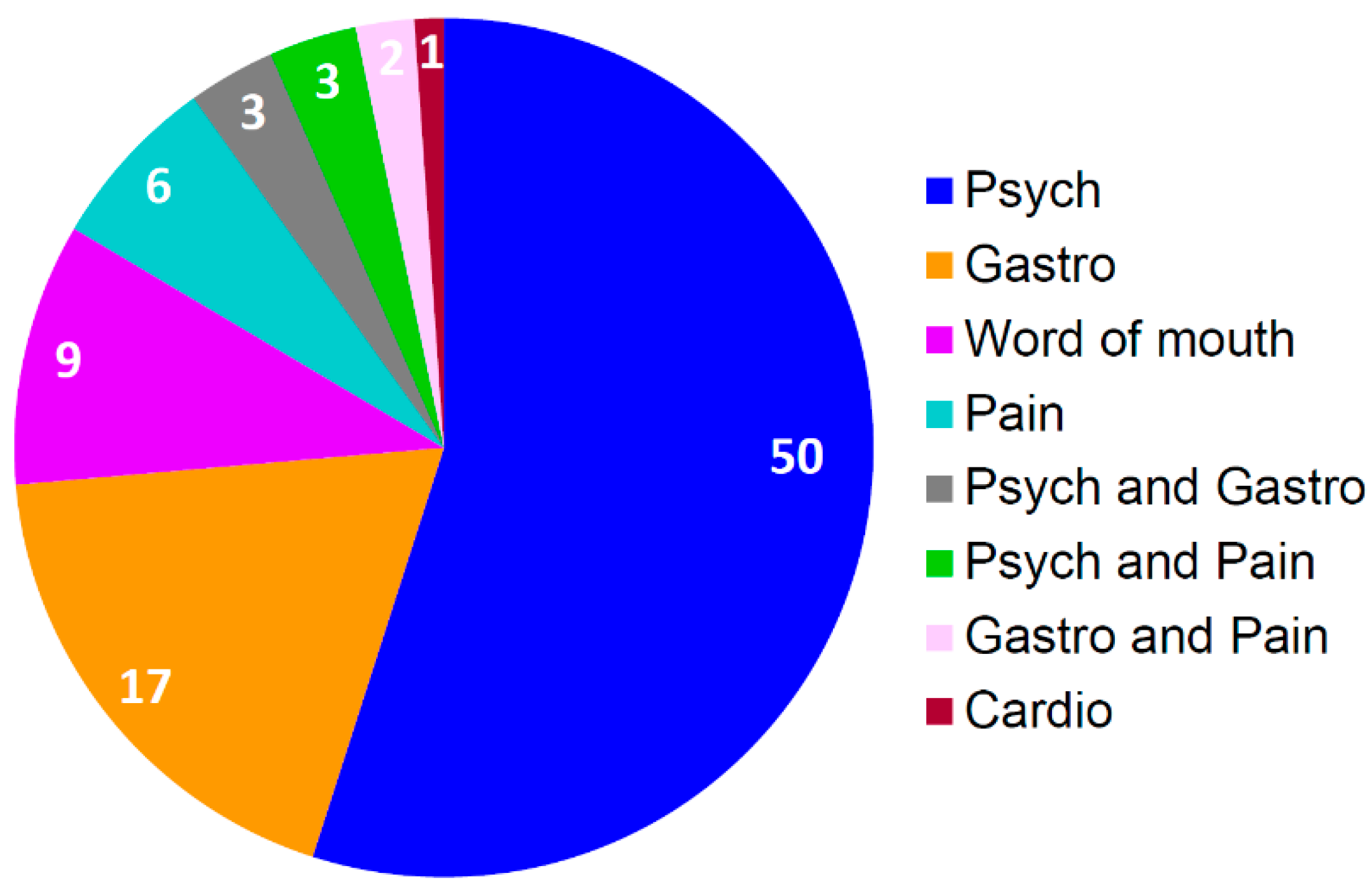
3.2. Operational Metrics
3.3. Clinical Metrics
4. Discussion
4.1. Successes
4.2. Challenges
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Green, J.S.; O’Brien, T.J.; Chiappinelli, V.A.; Harralson, A.F. Pharmacogenomics instruction in US and Canadian medical schools: Implications for personalized medicine. Pharmacogenomics 2010, 11, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Salari, K.; Karczewski, K.J.; Hudgins, L.; Ormond, K.E. Evidence that personal genome testing enhances student learning in a course on genomics and personalized medicine. PLoS ONE 2013, 8, e68853. [Google Scholar] [CrossRef]
- Calinski, D.M.; Kisor, D.F. An Interdisciplinary Experience focused on Pharmacogenetics: Engaging pharmacy and physician assistant students in conversations about antiplatelet therapy with respect to CYP2C19 genotype. Inov. Pharm. 2016, 7, 1. [Google Scholar] [CrossRef]
- Haga, S.B.; Mills, R.; Aucoin, J.; Taekman, J. Interprofessional education for personalized medicine through technology-based learning. Pers. Med. 2015, 12, 237–243. [Google Scholar] [CrossRef]
- Luzum, J.A.; Luzum, M.J. Physicians’ attitudes toward pharmacogenetic testing before and after pharmacogenetic education. Pers. Med. 2016, 13, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Press, K.R.; Bodurtha, J. Milestones for medical students completing a clinical genetics elective. Genet. Med. 2017, 19, 236–239. [Google Scholar] [CrossRef]
- Cavallari, L.H.; Pratt, V.M. Building Evidence for Clinical Use of Pharmacogenomics and Reimbursement for Testing. Adv. Mol. Pathol. 2018, 1, 125–134. [Google Scholar] [CrossRef]
- Johnson, J.A.; Weitzel, K.W. Advancing Pharmacogenomics as a Component of Precision Medicine: How, Where, and Who? Clin. Pharm. Ther. 2016, 99, 154–156. [Google Scholar] [CrossRef] [Green Version]
- Crews, K.R.; Cross, S.J.; McCormick, J.N.; Baker, D.K.; Molinelli, A.R.; Mullins, R.; Relling, M.V.; Hoffman, J.M. Development and implementation of a pharmacist-managed clinical pharmacogenetics service. Am. J. Health Syst. Pharm. 2011, 68, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Hicks, J.K.; Stowe, D.; Willner, M.A.; Wai, M.; Daly, T.; Gordon, S.M.; Lashner, B.A.; Parikh, S.; White, R.; Teng, K.; et al. Implementation of Clinical Pharmacogenomics within a Large Health System: From Electronic Health Record Decision Support to Consultation Services. Pharmacotherapy 2016, 36, 940–948. [Google Scholar] [CrossRef]
- O’Donnell, P.H.; Bush, A.; Spitz, J.; Danahey, K.; Saner, D.; Das, S.; Cox, N.J.; Ratain, M.J. The 1200 patients project: Creating a new medical model system for clinical implementation of pharmacogenomics. Clin. Pharm. Ther. 2012, 92, 446–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulley, J.M.; Denny, J.C.; Peterson, J.F.; Bernard, G.R.; Vnencak-Jones, C.L.; Ramirez, A.H.; Delaney, J.T.; Bowton, E.; Brothers, K.; Johnson, K.; et al. Operational implementation of prospective genotyping for personalized medicine: The design of the Vanderbilt PREDICT project. Clin. Pharm. Ther. 2012, 92, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuldiner, A.R.; Palmer, K.; Pakyz, R.E.; Alestock, T.D.; Maloney, K.A.; O’Neill, C.; Bhatty, S.; Schub, J.; Overby, C.L.; Horenstein, R.B.; et al. Implementation of pharmacogenetics: The University of Maryland Personalized Anti-platelet Pharmacogenetics Program. Am. J. Med. Genet. C Semin. Med. Genet. 2014, 166C, 784. [Google Scholar] [CrossRef] [Green Version]
- Cavallari, L.H.; Weitzel, K.W.; Elsey, A.R.; Liu, X.; Mosley, S.A.; Smith, D.M.; Staley, B.J.; Winterstein, A.G.; Mathews, C.A.; Franchi, F.; et al. Institutional profile: University of Florida Health Personalized Medicine Program. Pharmacogenomics 2017, 18, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Schuh, M.J.; Crosby, S. Description of an Established, Fee-for-Service, Office-Based, Pharmacist-Managed Pharmacogenomics Practice. Sr. Care Pharm. 2019, 34, 660–668. [Google Scholar] [CrossRef]
- Weitzel, K.W. Implementing pharmacogenetics in the clinical setting and competencies for health care professionals. In Pharmacogenomics: Applications to Patient Care, 3rd ed.; American College of Clinical Pharmacy: Lenexa, KS, USA, 2015. [Google Scholar]
- Dressler, L.G.; Bell, G.C.; Abernathy, P.M.; Ruch, K.; Denslow, S. Implementing pharmacogenetic testing in rural primary care practices: A pilot feasibility study. Pharmacogenomics 2019, 20, 433–446. [Google Scholar] [CrossRef]
- Dunnenberger, H.M.; Biszewski, M.; Bell, G.C.; Sereika, A.; May, H.; Johnson, S.G.; Hulick, P.J.; Khandekar, J. Implementation of a multidisciplinary pharmacogenomics clinic in a community health system. Am. J. Health Syst. Pharm. 2016, 73, 1956–1966. [Google Scholar] [CrossRef]
- Lemke, A.A.; Hulick, P.J.; Wake, D.T.; Wang, C.; Sereika, A.W.; Yu, K.D.; Glaser, N.S.; Dunnenberger, H.M. Patient perspectives following pharmacogenomics results disclosure in an integrated health system. Pharmacogenomics 2018, 19, 321–331. [Google Scholar] [CrossRef]
- Arwood, M.J.; Chumnumwat, S.; Cavallari, L.H.; Nutescu, E.A.; Duarte, J.D. Implementing Pharmacogenomics at Your Institution: Establishment and Overcoming Implementation Challenges. Clin. Transl. Sci. 2016. [Google Scholar] [CrossRef]
- Weitzel, K.W.; Duong, B.Q.; Arwood, M.J.; Owusu-Obeng, A.; Abul-Husn, N.S.; Bernhardt, B.A.; Decker, B.; Denny, J.C.; Dietrich, E.; Gums, J.; et al. A stepwise approach to implementing pharmacogenetic testing in the primary care setting. Pharmacogenomics 2019, 20, 1103–1112. [Google Scholar] [CrossRef]
- Relling, M.V.; Klein, T.E. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin. Pharm. Ther. 2011, 89, 464–467. [Google Scholar] [CrossRef]
- Swen, J.J.; Nijenhuis, M.; de Boer, A.; Grandia, L.; Maitland-van der Zee, A.H.; Mulder, H.; Rongen, G.A.; van Schaik, R.H.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From bench to byte--an update of guidelines. Clin. Pharm. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharm. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef]
- Weitzel, K.W.; Alexander, M.; Bernhardt, B.A.; Calman, N.; Carey, D.J.; Cavallari, L.H.; Field, J.R.; Hauser, D.; Junkins, H.A.; Levin, P.A.; et al. The IGNITE network: A model for genomic medicine implementation and research. BMC Med. Genom. 2016, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicali, E.J.; Weitzel, K.W.; Elsey, A.R.; Orlando, F.A.; Vinson, M.; Mosley, S.; Smith, D.M.; Davis, R.; Drum, L.; Estores, D.; et al. Challenges and lessons learned from clinical pharmacogenetic implementation of multiple gene-drug pairs across ambulatory care settings. Genet. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Haga, S.B.; Burke, W.; Ginsburg, G.S.; Mills, R.; Agans, R. Primary care physicians’ knowledge of and experience with pharmacogenetic testing. Clin. Genet. 2012, 82, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.M.; Weitzel, K.W.; Elsey, A.R.; Langaee, T.; Gong, Y.; Wake, D.T.; Duong, B.Q.; Hagen, M.; Harle, C.A.; Mercado, E.; et al. CYP2D6-guided opioid therapy improves pain control in CYP2D6 intermediate and poor metabolizers: A pragmatic clinical trial. Genet. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.K.; Bishop, J.R.; Sangkuhl, K.; Muller, D.J.; Ji, Y.; Leckband, S.G.; Leeder, J.S.; Graham, R.L.; Chiulli, D.L.; LLerena, A.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin. Pharm. Ther. 2015, 98, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Klein, T.E.; Caudle, K.E.; Haidar, C.E.; Shen, D.D.; Callaghan, J.T.; Sadhasivam, S.; et al. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin. Pharm. Ther. 2014, 95, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Cicali, E.J.; Blake, K.; Gong, Y.; Mougey, E.B.; Al-Atrash, H.; Chambers, N.; Denham, J.; Evans, J.; George, D.E.; Gomez, R.; et al. Novel Implementation of Genotype-Guided Proton Pump Inhibitor Medication Therapy in Children: A Pilot, Randomized, Multisite Pragmatic Trial. Clin. Transl. Sci. 2018. [Google Scholar] [CrossRef] [Green Version]
- El Rouby, N.; Lima, J.J.; Johnson, J.A. Proton pump inhibitors: From CYP2C19 pharmacogenetics to precision medicine. Expert Opin. Drug Metab. Toxicol. 2018, 14, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.; Voora, D.; Peyser, B.; Haga, S.B. Delivering pharmacogenetic testing in a primary care setting. Pharmgenomics Pers. Med. 2013, 6, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Marrero, R.J.; Cicali, E.J.; Arwood, M.J.; Eddy, E.; DeRemer, D.; Ramnaraign, B.H.; Daily, K.C.; Jones, D., Jr.; Cook, K.J.; Cavallari, L.H.; et al. How to Transition from Single-Gene Pharmacogenetic Testing to Preemptive Panel-Based Testing: A Tutorial. Clin. Pharmacol. Ther. 2020. [Google Scholar] [CrossRef] [PubMed]
- USA Food and Drug Administration. Drug Development and Drug Interactions: Table of Substrates, Inhibitors and Inducers. Available online: http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm (accessed on 1 December 2019).
- Storelli, F.; Matthey, A.; Lenglet, S.; Thomas, A.; Desmeules, J.; Daali, Y. Impact of CYP2D6 Functional Allelic Variations on Phenoconversion and Drug-Drug Interactions. Clin. Pharm. Ther. 2018, 104, 148–157. [Google Scholar] [CrossRef]
- Bahar, M.A.; Setiawan, D.; Hak, E.; Wilffert, B. Pharmacogenetics of drug-drug interaction and drug-drug-gene interaction: A systematic review on CYP2C9, CYP2C19 and CYP2D6. Pharmacogenomics 2017, 18, 701–739. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.A.; Sangkuhl, K.; Stein, C.M.; Hulot, J.S.; Mega, J.L.; Roden, D.M.; Klein, T.E.; Sabatine, M.S.; Johnson, J.A.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin. Pharm. Ther. 2013, 94, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Bell, G.C.; Caudle, K.E.; Whirl-Carrillo, M.; Gordon, R.J.; Hikino, K.; Prows, C.A.; Gaedigk, A.; Agundez, J.; Sadhasivam, S.; Klein, T.E.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin. Pharm. Ther. 2017, 102, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Pharmacogenomics Knowledge Base (PharmGKB) and Clinical Pharmacogenetics Implementation Consortium (CPIC). Gene-specific Information Tables for CYP2C19: CYP2C19 Frequency Table. Available online: https://api.pharmgkb.org/v1/download/file/attachment/CYP2C19_frequency_table.xlsx (accessed on 1 March 2020).
- Pharmacogenomics Knowledge Base (PharmGKB) and Clinical Pharmacogenetics Implementation Consortium (CPIC). Gene-specific Information Tables for CYP2D6: CYP2D6 Frequency Table. Available online: https://api.pharmgkb.org/v1/download/file/attachment/CYP2D6_frequencies.xlsx (accessed on 16 November 2018).
- Rosenberg, N.A.; Mahajan, S.; Ramachandran, S.; Zhao, C.; Pritchard, J.K.; Feldman, M.W. Clines, clusters, and the effect of study design on the inference of human population structure. PLoS Genet. 2005, 1, e70. [Google Scholar] [CrossRef]
- Rosenberg, N.A.; Pritchard, J.K.; Weber, J.L.; Cann, H.M.; Kidd, K.K.; Zhivotovsky, L.A.; Feldman, M.W. Genetic structure of human populations. Science (New York) 2002, 298, 2381–2385. [Google Scholar] [CrossRef] [Green Version]
- El Rouby, N.; Alrwisan, A.; Langaee, T.; Lipori, G.; Angiolillo, D.J.; Franchi, F.; Riva, A.; Elsey, A.; Johnson, J.A.; Cavallari, L.H.; et al. Clinical Utility of Pharmacogene Panel-Based Testing in Patients Undergoing Percutaneous Coronary Intervention. Clin. Transl. Sci. 2020, 13, 473–481. [Google Scholar] [CrossRef]
- Weitzel, K.W.; Elsey, A.R.; Langaee, T.Y.; Burkley, B.; Nessl, D.R.; Obeng, A.O.; Staley, B.J.; Dong, H.J.; Allan, R.W.; Liu, J.F.; et al. Clinical pharmacogenetics implementation: Approaches, successes, and challenges. Am. J. Med. Genet. C Semin. Med. Genet. 2014, 166, 56–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousman, C.A.; Arandjelovic, K.; Mancuso, S.G.; Eyre, H.A.; Dunlop, B.W. Pharmacogenetic tests and depressive symptom remission: A meta-analysis of randomized controlled trials. Pharmacogenomics 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperber, N.R.; Carpenter, J.S.; Cavallari, L.H.; Damschroder, L.J.; Cooper-DeHoff, R.M.; Denny, J.C.; Ginsburg, G.S.; Guan, Y.; Horowitz, C.R.; Levy, K.D.; et al. Challenges and strategies for implementing genomic services in diverse settings: Experiences from the Implementing GeNomics In pracTicE (IGNITE) network. BMC Med. Genom. 2017, 10, 35. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operational Metrics | Definitions/Examples/Comments |
|---|---|
| Number of referrals by general IM physicians | Total, by month |
| Types of referrals by general IM physicians |
|
| Number of referred patients lost to F/U, with reason | Example reasons: patient was unable to be contacted, patient decided against scheduling (e.g., cost, time, transportation) |
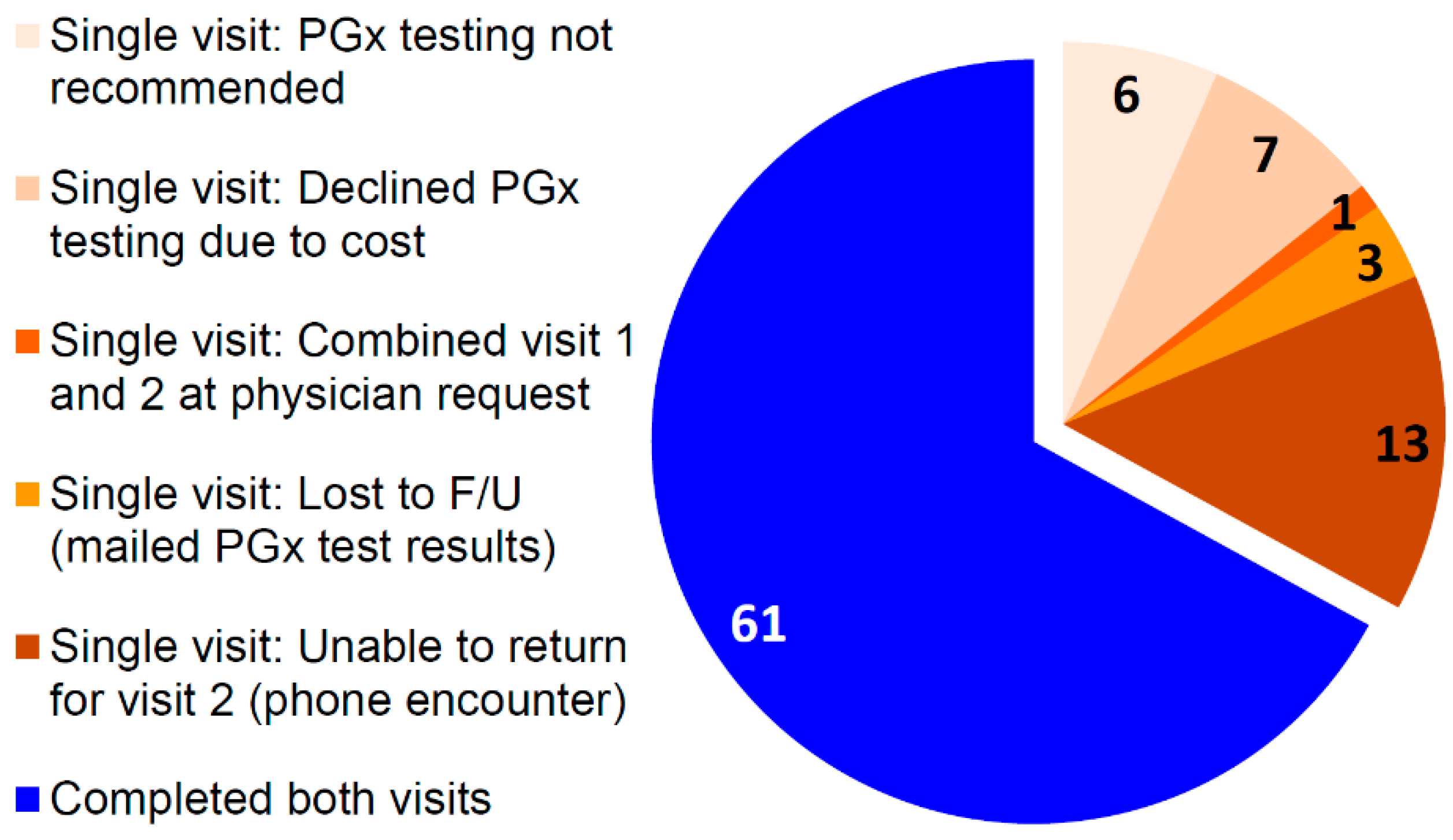
| Number of patients completing one or two visits, including reason for completion of single visit | Example reasons for completion of only single visit:
|
| Visit length | Approximate, in minutes |
| Number of patients recommended to receive and advised against PGx testing (with reason) 1 | Example reasons why patients were advised against testing: patient was responding appropriately to or not currently taking medications with CYP2C19/CYP2D6 evidence |
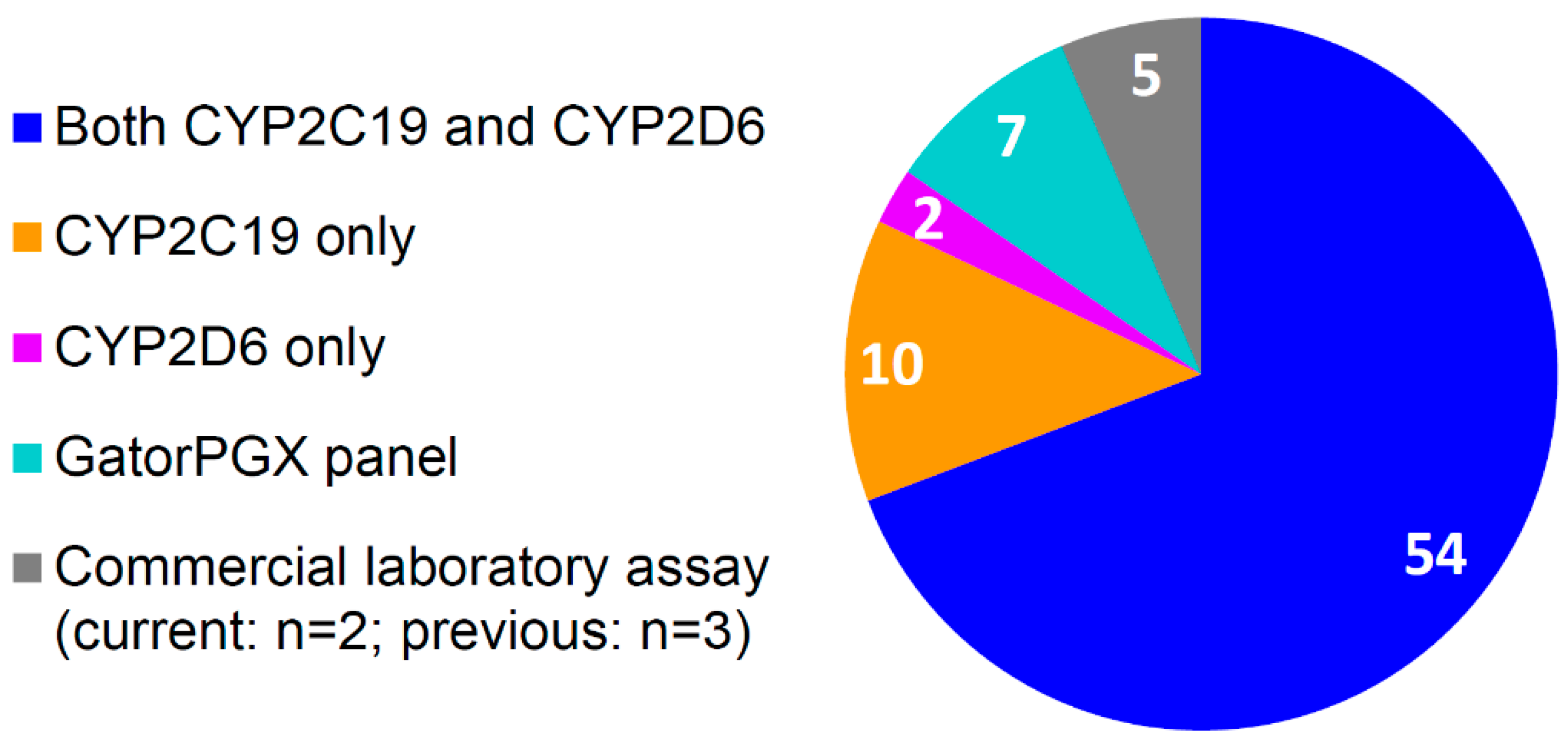
| Number of patients with PGx tests ordered 1, including test type | Types: name of gene or assay of PGx test (e.g., CYP2C19, CYP2D6, CYP2C19 and CYP2D6, GatorPGx panel [i.e., 9 pharmacogene panel offered by internal lab, Table S1]) |
| Number of patients who refused PGx testing, including reason 1 | Example reasons: cost, privacy concerns, unsure of value |
| Genotyping acceptance rate by patient | = |
| Number of patients with previously ordered PGx testing 1 | Included whether the PGx test met internal established criteria (described in text above) or whether the patient had to repeat testing |
| PGx test turnaround time | Time between sample collection and result being placed in the electronic health record |
| Clinical Metrics | Definitions/Examples/Comments |
| Patient demographics | Age, sex, race/ethnicity |
| Number of patients referred for guidance on one medication but pharmacist identified other medications that could potentially be impacted by CYP2C19/CYP2D6 | Example: Of the patients referred solely for psychiatric medication guidance, X% were taking at least one other medication that could be impacted by CYP2C19 or CYP2D6 (X% PPI, X% CYP2D6-guided opioid, X% clopidogrel).
|
| Pharmacogenetic test results | CYP2C19 and/or CYP2D6 genotype and phenotype per lab; determined predicted phenotype based on drug interactions (Table S2) |
| Number of patients on moderate and/or strong CYP2D6 inhibitor [35] | Moderate CYP2D6 inhibitor: duloxetine, mirabegron Strong CYP2D6 inhibitor: bupropion, paroxetine, fluoxetine |
| Number of patients taking/planning to take 2 genotype-guided medication | Genotype-guided medications: Current/ planned 2 medications that could be impacted by CYP2C19 and/or CYP2D6 per CPIC and/or DPWG guidelines [23,29,30,38,39]:
|
| Number and names of genotype-guided medications (visit 1) | |
| Number of patients with at least one actionable phenotype | Actionable phenotype: Phenotype warranting change in prescribing, dependent on gene-drug pair, as defined by CPIC and/or DPWG [23,29,30,38,39] |
| Number of patients with a recommendation to modify a dose or change a medication | Included recommendations pertaining to genotype-guided medications and medications relating to referral type (e.g., H2 receptor antagonist for patient referred for uncontrolled GERD/ lack of PPI effectiveness) |
| Number/type of recommendations | Type: New medication, alternative medication, discontinue medication, dose change ↑↓ |
| Recommendation acceptance rate | =
|
| CYP2D6-Guided Opioid (i.e., Codeine, Tramadol, Hydrocodone, Oxycodone) | SSRI | PPI | Any of These Medications |
|---|---|---|---|
| 4015 (42.6%) | 1955 (20.7%) | 2985 (31.7%) | 5445 (57.8%) |
| Characteristics | N = 91 |
|---|---|
| Age, years | 57 ± 18 |
| Sex, female | 61 (67.0) |
| Race/ethnicity | |
| European American | 83 (91.2) |
| African American | 3 (3.3) |
| LatinX | 2 (2.2) |
| Unspecified | 2 (2.2) |
| Native Hawaiian/Pacific Islander | 1 (1.1) |
| CYP2C19 Phenotype | PGx Clinic Patients 2 (n = 76) | European Reference Population [40,42,43] |
| UM | 6 (7.9) | 4.7 |
| RM | 22 (28.9) | 27.2 |
| NM | 23 (30.3) | 39.6 |
| IM | 20 (26.3) | 26.0 |
| PM | 5 (6.6) | 2.4 |
| CYP2D6 Phenotype | PGx Clinic Patients 3 (n = 68) | European Reference Population [41,42,43] |
| UM | 2 (2.9) | 3.3 |
| NM-UM | 3 (4.4) | 1.1 |
| NM | 48 (70.6) | 74.9 |
| IM | 6 (8.8) | 7.2 |
| PM | 8 (11.8) | 6.1 |
| Indeterminate | 1 (1.5) | 7.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arwood, M.J.; Dietrich, E.A.; Duong, B.Q.; Smith, D.M.; Cook, K.; Elchynski, A.; Rosenberg, E.I.; Huber, K.N.; Nagoshi, Y.L.; Wright, A.; et al. Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic. J. Clin. Med. 2020, 9, 2274. https://doi.org/10.3390/jcm9072274
Arwood MJ, Dietrich EA, Duong BQ, Smith DM, Cook K, Elchynski A, Rosenberg EI, Huber KN, Nagoshi YL, Wright A, et al. Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic. Journal of Clinical Medicine. 2020; 9(7):2274. https://doi.org/10.3390/jcm9072274
Chicago/Turabian StyleArwood, Meghan J., Eric A. Dietrich, Benjamin Q. Duong, D. Max Smith, Kelsey Cook, Amanda Elchynski, Eric I. Rosenberg, Katherine N. Huber, Ying L. Nagoshi, Ashleigh Wright, and et al. 2020. "Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic" Journal of Clinical Medicine 9, no. 7: 2274. https://doi.org/10.3390/jcm9072274